At 2:13 a.m., the hotel room is quiet—until it isn’t. One person is out cold after a day of delayed flights and back-to-back meetings. The other is wide awake, scrolling sleep gadget reviews and quietly bargaining with the universe: “If I can just get three solid hours, I’ll stop making jokes about your snore.”
That mix of travel fatigue, workplace burnout, and relationship humor is exactly why snoring is showing up everywhere right now. People want quick fixes, but they also want solutions that actually improve sleep quality. An anti snoring mouthpiece is one of the most talked-about tools because it’s simple, portable, and doesn’t require a full tech setup.
What people are buzzing about (and why it matters)
Snoring content has shifted from “funny problem” to “sleep health issue.” You’ll see it in the same feeds as smart rings, sunrise alarms, nasal strips, and mouth-taping debates. There’s also renewed interest in devices being tested in research settings, including a New clinical trial will test innovative anti-snoring device to tackle sleep disruption—a sign that sleep disruption from snoring is being taken seriously.
At the same time, mainstream guides keep repeating a practical message: start with basics, then choose tools that match the cause. That’s where mouthpieces enter the chat, along with broader conversations about sleep apnea and when snoring is more than “just noise.”
What matters medically (without overcomplicating it)
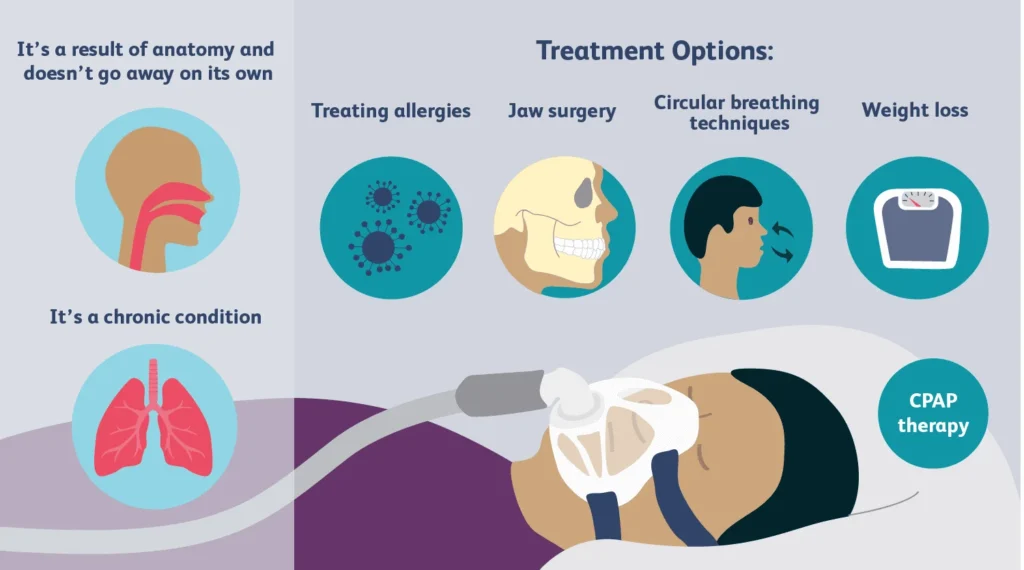
Snoring happens when airflow becomes partially blocked and soft tissues vibrate. Lots of things can narrow the airway at night. Common themes include sleep position, nasal congestion, alcohol close to bedtime, and changes in muscle tone during deeper sleep.
Snoring can also overlap with sleep apnea, a condition involving repeated breathing interruptions. Not everyone who snores has sleep apnea, but loud, habitual snoring paired with choking/gasping, witnessed breathing pauses, or heavy daytime sleepiness is a red flag.
Why sleep quality takes the hit
Even when the snorer “feels fine,” the bed partner may get fragmented sleep. In some cases, the snorer’s own sleep can become lighter and less restorative. That’s why couples often end up negotiating pillows, schedules, or separate rooms—then searching for something that actually reduces the sound.
What you can try at home (tools + technique)
If you want a realistic, low-drama plan, combine simple habit changes with a device you can tolerate. Comfort and consistency matter more than a perfect-looking gadget.
Step 1: Do a quick pattern check
- Timing: Is it worse after alcohol or a late meal?
- Position: Is it louder on the back vs. the side?
- Nose: Is congestion driving mouth-breathing?
- Energy: Any morning headaches or daytime sleepiness?
Step 2: Try the “ICI” basics: fit, comfort, and routine
Think of mouthpiece success like ICI: Insertion, Comfort, and Integration into your nightly routine.
- Insertion (fit basics): Follow the fitting instructions exactly. If it’s a boil-and-bite style, don’t rush the molding step. A sloppy mold often feels bulky and can trigger gagging.
- Comfort (pressure and positioning): A mouthpiece should feel snug, not like it’s forcing your jaw. Mild awareness can be normal early on. Sharp pain, numbness, or lasting jaw soreness is not.
- Integration (make it stick): Pair it with a simple routine: brush, rinse device, insert, then lights out. Consistency helps your body adapt faster.
Step 3: Pair it with positioning
Many people snore more on their back. Side-sleeping strategies can be low-tech: a supportive pillow, a body pillow, or a gentle “don’t roll over” setup. If a mouthpiece helps reduce airway collapse and you also stay off your back, you may get a stronger result than either approach alone.
Step 4: Don’t skip cleanup (it affects comfort)
A device that tastes weird or feels grimy won’t last long in your routine. Rinse it after use. Clean it gently with mild soap and a soft brush, then air-dry. Replace it if it warps, cracks, or won’t stay clean.
Where an anti-snoring mouthpiece fits
Most anti-snoring mouthpieces are designed to support the airway by changing jaw or tongue position during sleep. They’re popular because they travel well, don’t need charging, and can be less disruptive than some alternatives.
If you’re comparing choices, start here: anti snoring mouthpiece. Focus on comfort, adjustability (if available), and clear instructions for fitting and care.
When it’s time to stop DIY and get help
Snoring becomes a medical conversation when symptoms suggest sleep apnea or another sleep-breathing disorder. Don’t tough it out if you notice any of the following:
- Gasping, choking, or witnessed pauses in breathing
- Significant daytime sleepiness, dozing while driving, or “can’t stay awake” fatigue
- Morning headaches, dry mouth, or waking unrefreshed most days
- High blood pressure or heart risk factors alongside loud snoring
A clinician can help determine whether a mouthpiece is appropriate, whether a different approach is safer, and whether testing is warranted.
FAQ: quick answers people want before buying
Is a mouthpiece the same as a mouthguard?
Not always. Some products are designed for snoring, while others are for teeth grinding. The design and goal can differ.
What if I have a strong gag reflex?
Look for a lower-profile design and prioritize careful fitting. If you can’t tolerate it after a fair trial, consider other options.
Can I use one if I have dental work?
It depends. Crowns, bridges, aligners, and TMJ issues can change what’s safe and comfortable. Ask a dental professional if you’re unsure.
Next step: get a quieter night without turning sleep into a project
You don’t need a dozen sleep gadgets to make progress. Start with the basics, then test one tool at a time so you can tell what’s helping.
How do anti-snoring mouthpieces work?
Medical disclaimer: This article is for general education only and is not medical advice. Snoring can have many causes, including conditions that require professional evaluation. If you have symptoms of sleep apnea or significant daytime sleepiness, talk with a qualified clinician.