At 2:13 a.m., someone nudges their partner and whispers, “Please… roll over.” The partner tries, fails, and the snoring ramps back up like a ringtone you can’t silence. By morning, both people are tired, a little irritated, and quietly worried about what it means.
That scene is common right now. Between sleep trackers, “smart” alarms, travel fatigue, and workplace burnout, people are paying attention to sleep quality in a new way. Snoring isn’t just a punchline anymore. It’s a signal worth checking.
The big picture: snoring is noise, but it’s also information
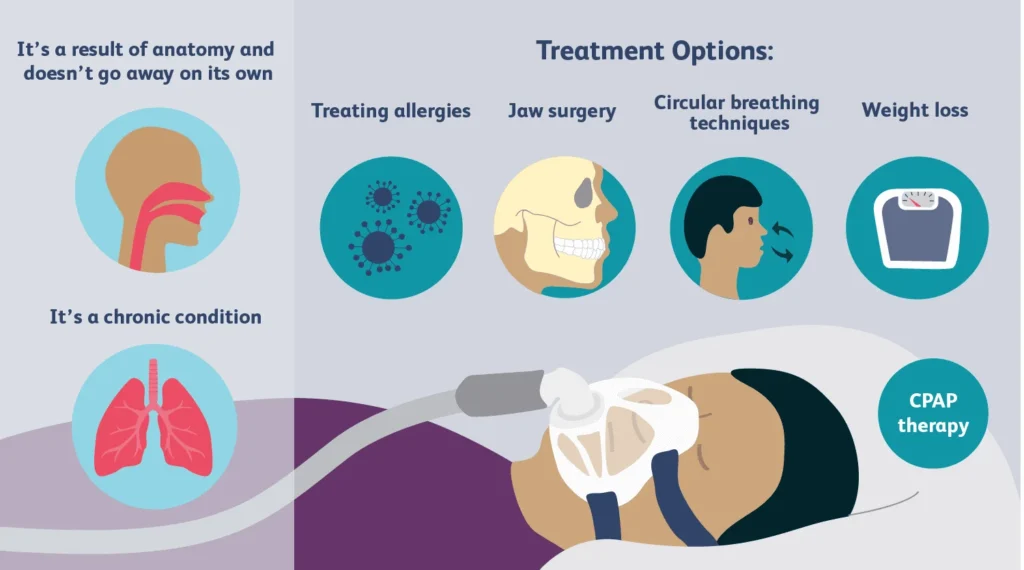
Snoring usually happens when airflow is partially blocked and soft tissues vibrate. Sometimes it’s tied to sleep position, nasal congestion, or alcohol close to bedtime. Other times, it can be linked to a more serious breathing issue during sleep.
That’s why recent coverage keeps circling one key point: snoring can overlap with sleep apnea warning signs. If you want a high-level overview from the news, see this related update: Snoring could be a sign of sleep apnea—see if this device can help.
Snoring also affects the person next to you. Broken sleep can show up as mood swings, lower patience, and more arguments about tiny things. That’s not “being dramatic.” It’s what sleep loss does.
The emotional part nobody wants to say out loud
Many couples treat snoring like a running joke. Then it turns into separate bedrooms, resentment, or that awkward moment when someone records the snore as “proof.” The snorer may feel embarrassed. The listener may feel lonely or trapped in a cycle of bad nights.
If this is you, aim for teamwork. Try: “I miss sleeping well next to you. Can we test a few options for two weeks?” That’s a shared goal, not a blame statement.
Practical next steps that don’t require a whole lifestyle overhaul
You don’t need to buy every sleep gadget on your feed. Start with simple, trackable changes. Keep it boring and measurable.
Step 1: Do a quick snore + sleep quality audit
- Timing: Did snoring get worse after a schedule change, travel, or daylight savings?
- Position: Is it louder on the back?
- Alcohol/sedatives: Did you have any close to bedtime?
- Nasal stuffiness: Are you congested or mouth-breathing?
- Daytime impact: Do you feel foggy, irritable, or unusually sleepy?
Step 2: Use sleep hygiene to reduce the “volume” of life
Campus health and sleep experts keep repeating the same basics because they work for many people. Stick to a consistent sleep window, keep the room cool and dark, and cut the doom-scrolling buffer before bed. If daylight savings throws you off, shift gradually when you can.
These steps won’t “cure” all snoring. They can improve sleep quality and make any snoring solution easier to evaluate.
Step 3: Where an anti snoring mouthpiece fits
An anti snoring mouthpiece is often designed to move the lower jaw slightly forward (a mandibular advancement style). That can help keep the airway more open for some people. It’s a popular option because it’s small, travel-friendly, and doesn’t require a battery.
Look for clear buyer guidance and verification steps, especially if you’re comparing brands that cite research or “consumer report” style claims. The goal is simple: a device you can actually wear comfortably and consistently.
If you want a product option that pairs jaw support with added stability, consider this: anti snoring mouthpiece.
Safety and testing: don’t ignore red flags
Snoring isn’t always harmless. Get medical advice promptly if you notice any of the following:
- Gasping, choking, or witnessed breathing pauses
- Severe daytime sleepiness or drowsy driving risk
- Morning headaches, high blood pressure concerns, or persistent brain fog
- Snoring that suddenly worsens without an obvious reason
What about mouth tape?
Mouth taping is trending in sleep content. It may sound simple, but it’s not a universal fix. If you have nasal obstruction, allergies, or possible sleep apnea, taping your mouth can be a bad idea. If you’re curious, talk to a clinician and prioritize solutions that keep breathing safe.
How to “test” a mouthpiece without guessing
- Pick a timeframe: Run a 10–14 night trial so you don’t overreact to one night.
- Track two outcomes: snoring intensity (partner rating or app) and your daytime energy.
- Watch your jaw: Mild soreness can happen early. Sharp pain, tooth pain, or bite changes should not be ignored.
- Keep variables steady: Don’t change caffeine, alcohol, and bedtime at the same time.
FAQs: quick answers people want before buying
Can an anti snoring mouthpiece stop snoring completely?
Sometimes it helps a lot, sometimes only a little. Results depend on why you snore, your fit, and whether you can wear it comfortably all night.
How do I know if my snoring might be sleep apnea?
Common red flags include loud snoring plus choking/gasping, witnessed breathing pauses, morning headaches, and heavy daytime sleepiness. A clinician or sleep test can confirm.
Is mouth tape a safer alternative to a mouthpiece?
Mouth tape is a trend, but it isn’t right for everyone and can be risky if you have nasal blockage or possible sleep apnea. Talk with a clinician if you’re unsure.
How long does it take to adjust to a mouthpiece?
Many people need several nights to a few weeks. Start with short wear periods and follow the product’s fitting instructions.
What side effects should I watch for?
Jaw soreness, tooth discomfort, gum irritation, dry mouth, or bite changes. Stop using it and get dental or medical advice if symptoms persist.
CTA: make it a two-week experiment, not a forever debate
If snoring is turning bedtime into a nightly negotiation, try a simple plan: pick one change, measure it, then decide. A well-fitted mouthpiece can be one of the most practical tools to test—especially when travel and stress already push sleep to the edge.
How do anti-snoring mouthpieces work?
Medical disclaimer: This article is for general education only and is not medical advice. Snoring can have many causes, including sleep apnea. If you have breathing pauses, choking/gasping, severe daytime sleepiness, or other concerning symptoms, seek evaluation from a qualified clinician.